Cleft lip and palate (CLP) and issues directly related to these anomalies, including
secondary deformities and velopharyngeal insufficiency (VPI). Cleft lip and palate
deformity can be distinguished from an isolated cleft palate (CP) on the basis of
epidemiologic, embryonic, and genetic factors. The etiology of cleft lip and
palate or cleft palate is believed to be multifactorial.
The scope of this field precludes in-depth discussion of surgical techniques and
controversies. Miscellaneous deformities, such as the Robin sequence, macroglossia,
ankyloglossia, and epignathus are briefly highlighted.
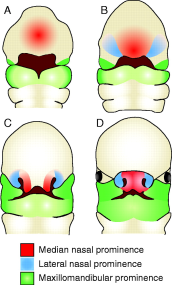
The image below depicts embryonic formation of the primary palate.
Illustration depicts fusion of the lateral nasal, medial nasal, and maxillary prominences
to form the primary palate.
Two thirds of all cases of clefting involve the lip with or without involvement
of the palate, whereas one third of all cases occur as an isolated deformity of
the palate. Males predominate within the cleft lip and palate (CLP) group (60-80%
of cases), whereas females constitute the majority within the cleft palate (CP)
group. Cleft lip and palate deformity is strongly associated with bilateral cleft
lips (CLs) (86% of cases); the association decreases to 68% with unilateral cleft
lip. The left side is most commonly involved in unilateral cleft lip cases.
Interracial differences exist in the incidence of cleft lip and palate versus cleft
palate. The mean incidence of cleft lip and palate is 2.1 cases per 1000 live births
among Asians, 1 case per 1000 live births among white people, and 0.41 cases per
1000 live births among black people. A high incidence of the cleft lip and palate
is seen in North American populations of Asian descent, such as Indians of the southwestern
United States and the west coast of Canada. The incidence of isolated cleft palate
is constant among the 3 racial groups at 0.5 cases per 1000 live births.
The incidence of cleft lip and palate also rises with increased parental age, and
older mothers with additional parity have an increased incidence of having children
with cleft palate.
In relatives of children with cleft lip and palate, the incidence of cleft lip and
palate is significantly increased. However, the isolated cleft palate anomaly occurs
with the same frequency as that in the general population. Relatives of children
with isolated cleft palate also have a higher risk of this anomaly, without an increased
risk of the cleft lip and palate deformity.
Overall, 5% of patients with cleft lip and palate and isolated cleft palate have
identifiable syndromes. Associated syndromes are more common among patients with
isolated cleft palate than among others.
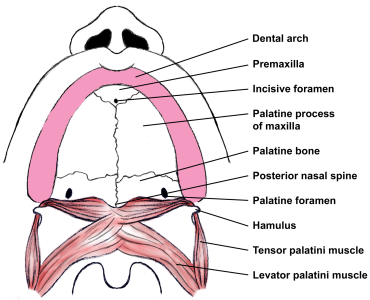
The following image depicts the normal palate anatomy.
Normal anatomy of the palate.