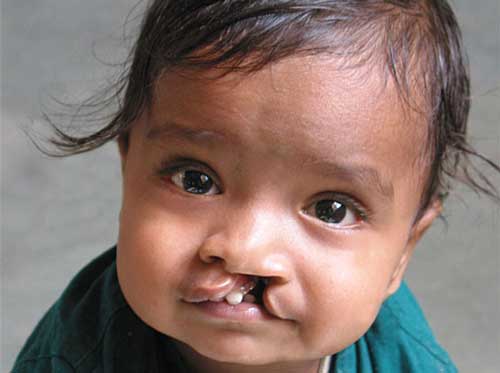
Did you know that the roof of the mouth (palate) is formed between
the sixth and ninth weeks of pregnancy. A cleft palate happens if the tissue that
makes up the roof of the mouth does not join together completely during pregnancy.
For some babies, both the front and back parts of the palate are open. For other
babies, only part of the palate is open.
Did you know that Cleft lip and/or palate is one of the most common
problems found in newborn babies.
Did you know that children with a cleft lip with or without a cleft
palate or a cleft palate alone often have problems with feeding and speaking clearly
and can have ear infections.
Did you know that children also might have hearing problems and
problems with their teeth.
Did you know thatthe causes of orofacial clefts among most infants
are unknown. Some children have a cleft lip or cleft palate because of changes in
their genes. Cleft lip and cleft palate are thought to be caused by a combination
of genes and other factors, such as things the mother comes in contact with in her
environment, or what the mother eats or drinks, or certain medications she uses
during pregnancy.
Did you know that Orofacial clefts, especially cleft lip with or
without cleft palate, can be diagnosed during pregnancy by a routine ultrasound.
They can also be diagnosed after the baby is born, especially cleft palate.
Did you know that sometimes certain types of cleft palate (for
example, submucous cleft palate and bifid uvula) might not be diagnosed until later
in life.
Did you know that treatment for children with orofacial clefts
can vary depending on the severity of the cleft; the child’s age and needs; and
the presence of associated syndromes or other birth defects, or both.
Did you know that surgery to repair a cleft lip usually occurs
in the first few months of life and is recommended within the first 12 months of
life.
Did you know that surgery to repair a cleft palate is recommended
within the first 18 months of life or earlier if possible. Many children will need
additional surgical procedures as they get older.
Did you know that surgical repair can improve the look and appearance
of a child’s face and might also improve breathing, hearing, and speech and language
development.
Did you know that children born with orofacial clefts might need
other types of treatments and services, such as special dental or orthodontic care
or speech therapy.
Did you know that with treatment, most children with orofacial
clefts do well and lead a healthy life.
Did you know that some babies with clefts have very few or no problems
feeding, while others have more difficulty. Use of special bottles and careful positioning
of the baby are sometimes helpful modifications.
Did you know that there is no relationship between mental retardation
and cleft lip and palate. However, if the cleft is part of a cluster of other problems
(a syndrome), learning ability is sometimes affected.
Did you know that the more specialists participating on the team,
the more likely every aspect of treatment can be considered during the team evaluation.
The specific staff will be determined by the availability of qualified personnel
and by the types of patients served by the team.












[0]}})